Yeah, yeah bunions are a trendy topic and I’m cautiously hopping on the bandwagon to offer A perspective influenced by my training with Anatomy in Motion (fully disclosing my biases as an instructor).
Do I have anything new or groundbreaking to add to the bunion discussion? Nope.
Do I have any revolutionary evidence or new theories to prove the causative mechanism for bunion formation? Nope.
Do I really know anything? Not really.
Wish I knew who to credit this to…
In a perfect world, we’d want to understand what factors led to the bunion(s) forming in the first place… Shit footwear? “Genetics”? Repetitive poor movement of the body above? Previous injury? Probably a little bit of everything.
Regardless of the causal factors, it should be empowering to hear that there are some consistent mechanical findings that often go together with a bunion that you can start to address right away.
First, watch this:
As I describe in the above video, a common mechanical consistency with most buniony feet is that the joints posterior to the 1st MTPJ DO NOT GAP on the medial border of the foot and, instead, the big toe joint is doing allllll of the gapping (abduction). A good strategy would be to start to redistribute the gapping of the medial border across ALL joints, not just the one MTPJ.
I think some people call that load-sharing, a term most commonly used in reference to spine motion and can describe why some people have back pain.
Much like a spine with a hinge point at the thoracolumbar junction, through which all their extension is occurring, a foot with a “hinge point” at the 1st MTPJ, through which all their pronation is occurring can lead to a structural distortion over time that can become stiff and rigid and not super comfortable.
The intention of the exercise I demo in the video is to MINIMIZE the valgus/ABduction/ER/gapping (whatever you want to call it) motion of the big toe, and MAXIMIZE joint opening at the other joints on the medial border of your foot, encouraging healthy pronation mechanics with even joint motion distribution through the entire foot.
And if you understand that as a movement principle, you can get really creative with how you go about working with a bunion, or any part of the body.
What about toe spacers?
In the video, I am using the sock-between-the-toes technique in a way that is reminiscent of a toe spacer. But this is not meant to be a passive solution, like toe spacers often are portrayed as. The goal is use the sock as a tool to re-educate your foot to move differently. Not to hold all the toes apart 24/7 in hopes it will change foot mechanics. Like putting a book under your pillow hoping to learn passively in your sleep… I WISH it worked that way.
I’m sure there is a time and a place for toe spacers as a passive tool, but I’ve personally never recommended people to use them, nor have I ever used them myself (nor have I ever told anyone to STOP wearing toe spacers- Your feet, your choice). Except for a few times I painted my toe-nails…
I find the most repulsive thing about this photo to be the choice of polish colour. Bleh.
Here’s another creative set-up one of my clients came up with to redistribute her big toe’s excessive valgus to her forefoot and rearfoot:
The band is pulling her valgus big toe into ADduction (towards midline of the body), while she pronates her foot to encourage opening of the joints on the medial border of her foot without excessive big toe bunionization (that’s totally a word). The black AiM wedge is promoting inversion of her forefoot to further encourage healthy pronation mechanics.
Want to learn more?
If you are a manual therapy or movement practitioner and you’d like to learn more about foot mechanics in gait, I will be teaching an Anatomy in Motion Module 1 seminar on Sept 22-24 2023. If you are in the Greater Toronto Area, come nerd out!
This was a quick overview, not intended to be specific medical advice. If you are looking for help for your own body, it is important to receive individualized guidance for your body’s unique issues. Get a professional you trust to assess your unique needs, or get in touch if you’d like to work together to find movement-based solutions to help your body move and feel better.
Is your back issue coming from your foot? Or is your foot issue coming from your back? Ain’t no way to know until we assess! This blog post is dedicated to investigating this chicken-or-egg question.
Scroll down a little more to join me in a fantastic biomechanical nerd-out 😉
This blog post is for you if you currently have a stiff spine, stiff foot, long time back issue, old foot injury, all of the above, or are just curious about how to get your body moving more efficiently by learning about the movement relationship between your feet and spine.
You are more than the sum of your parts
I know you know this already, but it cannot be repeated enough: The body is a beautifully connected whole system, and should be considered for the whole that it is, not reduced to individual parts operating in isolation from each other.
One of my online students (a musician) recently wrote to me about how useful it has been, through doing my sessions regularly, to become more aware of all the various connections between her body parts in motion.
Like understanding that if you can’t move your big toe THIS way, then your hip is going to be restricted going THAT way, and maybe that’s why your left shoulder feels janky.
Janky: Junk + cranky. Technical term (which I stole from a client of mine, in reference to her janky shoulder).
I love discovering connections in the body, too. It really lights me up because it always leads to better flowing movement and less pain. This is the magic we tap into in studying Anatomy in Motion: How everything needs to coordinate with everything else for ideal gait.
But its not magic. Its biomechanics.
In the words of my wonderful mentor Gary Ward, creator of Anatomy in Motion: “Look for things that don’t move that give permission for other things to.”
That adds an additional layer of nuance to the stretch and strengthen conversation, doesn’t it??
And on this note, I’d like to share with you a series of video clips from my most recent Movement Deep Dive session: Foot-Spine Connections.
As the name alludes to, this session’s investigative mission is to learn if there is a discombobulated relationship between the movement of your feet and spine that could be keeping your body stuck moving inefficeintly through each footstep, with discomfort or whatever jankiness you’re aware of in your body.
Understanding this foot-spine connection is extremely useful when we are working on helping our bodies move and feel better with less pain, because it helps us to become aware of how the causative root of a foot issue could be your spine, or visa versa.
This helps us to make better informed choices about what we can focus on in our movement practices, instead of just trying random stuff and hoping for the best.
And so on that note, please enjoy these 4 snippets from the Foot-Jaw Connections Movement Deep Dive.
I hope you’ll be able to learn a little about how your feet and spine are moving, and how to restore ideal mechanics between the two structures to put more flow in each footstep.
Foot-Jaw Connections
So, how did stuff go? Did you discover anything new and useful? I’d love to hear how this little bit of movement detectivery went for you. Please write me a comment below if you’d like to share.
Obviously there is more to explore than this… But I hope to inspire you to use this way of thinking in all your movement endeavours. Think outside the box. Think of your body as more than the sum of it’s parts. Just… Think ;).
In the full session, we also explore new ways of moving that connect your feet and spine with each other to restore a more harmonious, flowing relationship. But I can’t share EVERYTHING for free, because this is capitalist America.
If you’d like to see the full 50ish minute movement deep dive session and participate along, you can find it listed HERE, along with some other faves, for $20 each.
If I had only 15 minutes with someone to help them move and stand with more ease, but was not allowed to assess anything or ask about their injury history, I think the most impactful thing to do would be…
Teach them how to pronate their feet.
Pronation is not the devil, but the devil is in the details.
I’m here about the pronation!
Pronation is an important motion the foot must be able to do as we walk. Contrary to what your orthotics person may have told you.
With each step, the foot gets just one chance to pronate. Could you missing out on the important benefits of this moment in time? (more about that below, read on!).
At some point in my work with most clients, I know I’ll do eventually take them through an exercise to show them how to access a healthy pronation, its just a matter of when.
I think that the world of therapy and movement professionals is opening up to the idea that pronation is a healthy movement to promote, with much thanks to the work of Gary Ward. Which is awesome.
However…
Just rolling your foot IN is not the same as pronation.
Do you know the difference?
Eversion (rolling onto the inside of your foot… I know, it seems like it should be called INversion, just deal with the counterintuitive language), is the frontal plane component of pronation, not the whole shebang.
My intention with this blog post is to highlight the diffrences between pronation and eversion of the foot, so that you can liberate your feet and wake up their muscles instead of living with a problematic chunk at the end of your leg.
So before you read any further, stop what you’re doing (unless you’re saving your baby from being eaten by a dog or something) and follow along with the video below. Let’s see how well your feet move. Are you just everting, or are you actually pronating?
The clip is from day 2 of my Liberated Body workshop: Foot mechanics day, in which we explore healthy pronation and supination of the foot.
In fact, embracing pronation is often the biggest take-away for my students. One said: “I was convinced that pronation was a horrible thing until this class!”
Pronation is a tri-planar movement
Eversion describes only the frontal plane aspect of pronation
The main difference between pronation and eversion, in super simple terms (because my brain needs things to be simple):
Do you roll inwards on your foot, dump your knee wayyy inside of your big toe, and lose contact with the 5th metatarsal head on the floor? That’s eversion of the whole foot, not pronation.
Check out these images:
Accurately labelled. Notice the loss of 5th met contact in the eversion photo, and likewise, the loss of 1st met contact in the inversion photo. No tripod, no pronation.
Yes, these are also labelled accurately: Notice how the calcaneus (heel bone) is rolling into eversion, but it appears that the whole foot tripod is still in contact with the ground. Got tripod? That’s a pronation.
Notice how the labels in brackets underneath that say pronation and supination are not accurate, because the foot is clearly rolling off the floor, losing tripod contact.
Are you doing the right thing the wrong way?
As with anything, attention to nuance is the key for success. We could be doing the “right” thing the wrong way,
Like when I first tried a low carb, high fat diet in 2013ish because that’s what the whole internet was doing… No one told me how easy it was to eat 12483275939 calories of fat a day and gain weight on a “fat-loss” diet. Oops.
Could you be thinking you’re pronating, but just smashing the shit out of your first met by dumping all your weight onto it, with no muscles managing the situation?
Here’s one more nuanced pronation “DO” and “DON’T” that I hope you picked up from my video: We DO want the knee to go slightly inward to access foot pronation, but we DON’T want the knee to dump inward so far it generates eversion.
Check out this video by Gary Ward (which he created to illustrate the concept from his book What the Foot, that knee over second toe is not a thing we should get dogmatically locked into because it limits foot movement in gait):
Here’s your pronation vs. eversion check-list for success:
Eversion:
No articulation between foot bones
Foot “log-rolls” inward as one chunk
Loss of tripod (5th metatarsal head lifts from floor)
No change in muscles length or experience loading/stretching under foot
Joints remain in same position, nothing decompresses/compresses
Pronation:
Articulation between the foot bones with each other and the ground
Tri-planar motion of the foot (sagittal, frontal, and transverse plane components- eversion is just the frontal plane component of pronation)
All three points of the tripod in contact with the floor
Muscles on the bottom and inside surfaces of foot, and back of the ankle load and lengthen
Joints on the bottom and inside surface of the foot open and decompress.
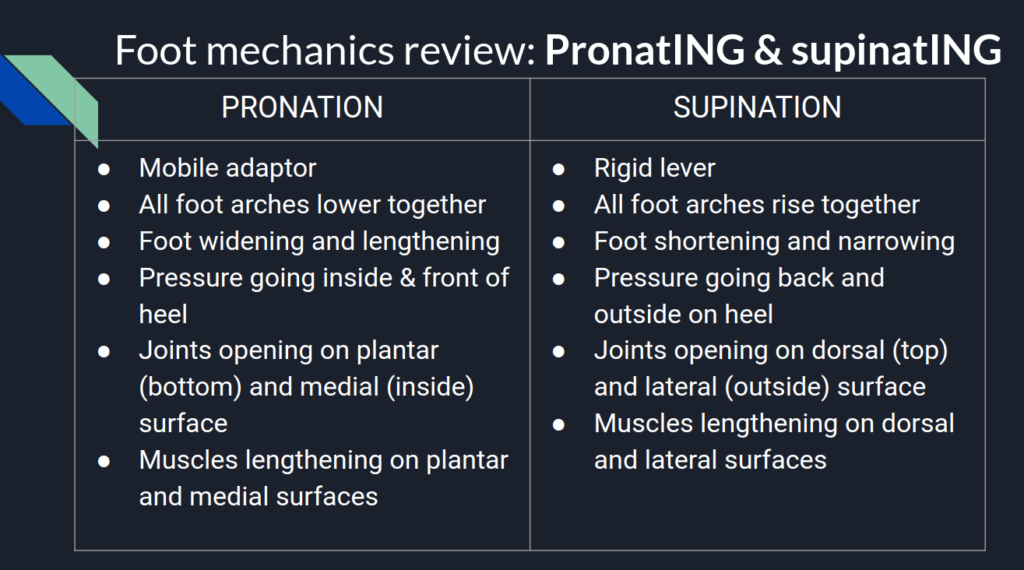
Here’s a slide from my Liberated Body workshop day 2 presentation that outlines what we’re looking for in healthy pronation and supination:
Why is pronation actually useful?
Just to clarify: PronatING is great. Being stuck in pronaTION, the noun, is not so great.
Pronation is like going to Wal-Mart- Get in, get what you need, and get out as quickly as possible.
Here are a three amazing things our body gets from healthy pronation (but does not get from rolling in, aka eversion):
Natural lengthening and loading of the muscles under the foot with each step: Got tight feet? Stretching not really helping? Rolling fascia out feels good, but not changing anything? Foot pronation is the movement that naturally allows the muscles under your foot to lengthen with each step. Got plantar fasciitis? Letting your feet pronate could be a game changer for you.
Extensor chain (dem glutes) load: Looking for more ease and power with each stride? Or to explode up from a squat position? Or land from a jump with more control? At the same moment in time that we pronate our foot in gait, the entire extensor chain of the lower body loads up. Calves load to generate plantarflexion, distal quads load to generate knee extension, and proximal glutes and hamstrings load to generate hip extension. Want to jump better and run with more ease? Make sure your feet can pronate well.
Pronation and eversion (rolling in on the foot) are not the same. One is a useful experience for the whole body, the other just feels uncomfortable.
Eversion is just one component (frontal plane) of a healthy, three dimensional pronation.
Losing the foot tripod makes or breaks a pronation. And a tea towel might be your new best friend.
Pronation has important movement repercussions for the body, such as allowing us to mobilize our feet naturally with each step, helping us engage our glutes better, and even freeing our neck and jaw tension.
Wal-Mart sucks.
Want to learn more?
I think you’ll really love Wake Your Feet Up, an online course by Gary Ward that teaches foot mechanics in a way that even my simple brain can comprehend.
He designed this course for folks who want to learn more about their foot mechanics and explore exercises to give their tootsies back their full movement potential. This online course is appropriate for all humans with feet, not just movement and therapy professionals who can speak biomechanics.
Ok I realize this post makes me seem like a huge Gary Ward fan-girl. I kinda am. Deal with it. I think he was my dad in a past life.
That’s all for now, movemet pals. I’d love to hear if you discovered anything new about your feet: Are you pronating well, or just everting? And if you can get your feet pronating well, what does it feel like for your feet, and the rest of your body?
Leave a comment, or shoot me an email, and let me know 🙂
Why do they form? What do you do about them? Can you do anything about them? Aren’t they genetic? Do you need to get surgery? What about those toe spacer things and splints?
So many questions!
I’m not claiming to have any conclusive answers (and I think the moment we conclude something is the moment we stop learning anything new).
But what I do know is that bunions can be understood and worked with from a movement perspective. That is, movement of the big toe created the bunion, why could movement not also be at least part of the remedy?
I believe movement is medicine. But too much medicince can be problematic too, can’t it?
Here’s a key thing to know: The movement of the big toe that leads to a bunion forming- toe abduction/valgus- happens at a specific moment in time in the gait cycle. Things get problematic when that movement becomes the only option your foot has and becomes a structural adaptation, ie, the actual shape of your foot changes.
The bunion itself is the solution your body found for a problem.
The video below is a clip from a Movement Deep Dive Session I did recently with some of my amazing Liberated Body students. The session was to help them understand big toe mechanics with foot pronation and supination as we walk.
I think knowledge is power… Wanna geek out?
In the video I cover:
What joint motions are possible at the big toe joint (aka 1st metatarsalphalangeal joint aka MTPJ)?
How is movement of the foot on the floor- closed chain- different than when it swings through the air- open chain?
What does the big toe do when the foot pronates and supinates?
What big toe/foot movement creates a bunion over time and when does that happen in gait?
How can a bunion be seen as an indicator to that we need to pronate that foot better?
How could this be affecting stuff above, like your neck?
When we understanding how the big toe moves in relationship with the foot and the rest of the body, we have powerful information to inform the decisions we make for our bodies everyday.
I hope the video demonstrates how the big toe movement that leads to a bunion forming- toe abduction- is a totally natural event with each step we take. We just want to have other options, too.
Interestingly, while bunions are association with a more pronated foot, the bunion may form because the foot doesn’t pronate well! The big toe abducting away from the foot was the last ditch attempt to do something that resembles pronation. I often find that if we show the foot how to pronate better without relying solely on the big toe deviating into excessive abduction, good things happen.
So if you have a bunion, maybe your big toe is just stuck in a moment in time because it only has one option for movement? What if you could show it a new option?
I think its safe to say that before electing for an invasive buinion procedure, or using a medieval-looking toe stretching devices, or shoving spacers between your toes, why not try some natural movement, first? Give that foot some of its movement potential back.
Best case scenario, you can get that toe moving again and things will feel better. Worst case, you mobilized your feet and got some extra bloodflow. Win win.
This is why I’m so passionate about the work Gary Ward teaches in his Anatomy in Motion courses. What if we could restore the movement potential inherent in our gait cycle, so that each step we take has the ability to reinforce healthy joint mehcanics? Walk ourselves well.
Want to learn more? I think you’ll really enjoy my four day workshop Liberated Body. We spend the whole of day two moving your feet 🙂 I have a live workshop every few months, and it’s also available as a home-study you can start today 🙂
In fact, here’s a story from one of my students, a dancer and yogi, who embraced pronating her feet and was able to free up her bunion:
“My most enjoyable class and the biggest change I noticed was in the FEET! I feel that I have avoided pronation like the plague which stems from ballet training for sure – but my feet, achilles, calves and even knees felt SO GREAT after that class. I purposefully went for a walk afterwards and could really feel a difference in my foot pressures as I moved. Also as I mentioned at the end of the session, my bunion on the right side felt released and not as painful – coming up to demi-pointe on that side was a breeze.”
Super cool, right!?
What do you think? Do you have bunions? Have you had a bunion surgery? Have you had success using movement to relieve bunion pain? I’d love to hear from you.
Leave a comment here, shoot me an email, or find me on the social media things you do. I’m pretty much the only Monika Volkmar on the planet, so I’m easy to find 😉
Alternative title: Foot pronation is not the devil.
If you don’t want to read this whole blog post (won’t take it personally, my posts can be long…) go to the bottom to watch an excerpt from an online movement session I did last week linking foot and jaw mechanics in gait.
Go with the flow (motion model)
About once a week I do a movement session with students who’ve completed my Liberated Body 4 day workshop. The intention is to help them deepen their understanding of how our bodies were designed to move based on the joint interactions taught in Gary Ward’s Anatomy in Motion, and his Flow Motion Model of the gait cycle.
I love this model (FMM) because it maps how any one part of the body is linked to all of others via their joint interactions through the gait cycle.
We can use the model as a map to identify the joint motions and interactions your body is having truoble accessing so we can give these sepcific things back to your system.
Peoples’ bodies tend to like feeling more complete.
I thought it would be nice to summarize one of my most recent online movement sessions in which we looked at the joint interactions that link movement of the foot with the jaw.
The very short story: Foot pronation couples with jaw decompression (mandible sliding forward and down from the temporal bones).
My invitation to you, if yo’re interested, is to come take this journey from your foot to your face. It’s fun. It’s logical. It will hopefully even be useful! (and check out the video at the end of this post to see a clip from the session to follow along with).
WHAT IS THE JAW?
Seems like an obvious question. However, I’ve made it my personal practice to never again take for granted that I understand what a joint is. Nor will I assume that the person I am talking to has the same understanding of a joint as mine.
I fondly recall the moment I actually understood what a shoulder was. It was just last year…
So when we say “jaw”, what’s the reference point? Are we talking about the mandible? The temporal mandibular joint (TMJ)? Where does the word jaw even come from?
I did a bit of etymological research and tfound that “jaw”, from mid 15th century old English referred to “holding and gripping part of an appliance”.
Holding and gripping… Sounds like what many of us do with our jaws today.
Your jaw is actually the “gripping” part of your face. Feels true, don’t it? 😉
The jaw has two articulating bones: Mandible + temporal bone.
In desribing the motion of the jaw, we’ll refer to the mandible’s movement interaction with the temporal bone.And we’ll consider the temporal mandibular joint- TMJ- as simply the space between the mandible and temporal bone. There’s a articular condyle in there. And some synovial fluid, too.
We’ll use the words protrusion (forward) and retrusion (backwards) to refer to mandibular motion in relation to the rest of the skull. And we’ll use the words compression and decompression to refer to the TMJ’s state of more or less pressure respectively.
As you open your mouth the mandible protrudes (slides anteriorally and inferiorally) opening space in the TMJ, and we’ll call it a decompression. And visa versa.
For purposes of this blog post, we’ll talk mostly sagittal plane (forward and back movement), but know that the mandible and TMJ have movement capacity in frontal and transverse plane- lateral shifts and rotations right and left. Not a lot, but enough to be significant.
Now the fun part… Your jaw has a specific way of interacting wiht the rest of the body as you walk.
All joint motions the body can do show up in gait. Even the jaw’s motions, though it is so subtle and happens too quickly to pay attention to it unelss you really focus.
Every single joint in the body has the opportunity to articulate to both ends of it’s available movement spectrum, in all three planes, with each foot step. Every movment your body can do it does in the space of 0.6-0.8 seconds with each step.
Unless it can’t.
So if a joint doesn’t have access to a movement just standing and trying to isolate it, you can bet it won’t be happening when you walk either. This leads to new strategies that are more effortful, and may lead to new problems later.
How does lack of movement at the foot affect the jaw? How does lack of movement at the jaw affect the foot?
The jaw is a DANGLER
In AiM, Gary has taught us to think of several structures as “danglers”.
The mandible is a dangler.
Because it dangles, it doesn’t really do much on its own accord as we walk, it just comes along for the ride. It doesn’t actually have inherent motion that contributes to gait, but think of it as needing to sway in harmony with its surrounding structures as part of a global mass-management strategy.
When the jaw gets stuck in one position and only has that one option, it can impact on the movement options for the rest of the body.
OCCLUSION, PROPRIOCEPTION, AND THE RETICULAR ACTIVATION SYSTEM
Occlusion refers to where the surfaces of the teeth touch. This can have an impact on whole body on movement potential.
In my early AiM days, I recall that I couldn’t find my hamstring load in the heel strike (hamstring “stretch”) exercise on my left leg.
Then I randomly came accross a chart with the teeth and their association to different muscles. I’ve misplaced said chart and all I remember was the connection between molars and hamstring (and if anyone has this or a similar chart I would love to see it!).
Just for the fun of it, I tried doing the heel strike exercise while holding contact with my left molars. BOOM hello hamstrings. Freaky biomechanical magic.
(If you want to learn more about heel strike and how the hamstrings load in gait, I recommend Gary Ward’s Lower Limb Biomechanics course. So good!)
It is also said that the jaw is said to contain the highest number of proprioceptors compared to any other area of the body. Meaning we get a ton of information about our body’s orietation in space from our jaw. And because we can’t see our own jaw, we probably oreint our body’s center of mass based on our jaw’s perceived center to some degree. (I am going to make a little video soon for you to play with this concept… stay tuned!).
Lastly, its good to know that the muscles of the jaw are supplied by the trigeminal nerve, which is closely related to the reticular activation system, which helps us filter information from our environment into categories of safe vs. unsafe, and is linked to states of anxiety, stress, anger, etc.
A curious personal observation is that on days when my bite is more centered, I’m usually in a brighter, cheery mood, full of optimism, and my body has less of my usual annoying symptoms. When my bite is off (usually shfited, laterally flexed, and rotated left), I’m likely to be more irrtable and triggerable by silly bullshit, and more of my symptoms may be present. N=1, but its been useful to pay attention to this.
All this to say, TMJ mechanics and resting bite can have an effect on how we move and how we feel. So we want it to be able to dangle freely, in the right relationship with the rest of the body, which should happen in a particular way with each step we take.
“DEMONIZED” MOVEMENTS THAT COUPLE WITH JAW DECOMPRESSION
What happens when we start labelling one movement “good” and another bad”? We avoid the bad ones and do more of the good ones. This may be conscious or unconscious.
Either way, avoidance of a movement is problematic because no joint motion in the body happens in isolation, but in relationship with everything else.
In gait, if one joint moves, every joint moves.
So when I ask your foot to pronate, I’m actually asking your whole body to pronate with it- A foot pronation accompanied by all the other joint motions that should happen at the same snapshot in time at which the foot pronates in gait.
Have you been taught that pronating your feet was bad? I was. Like, hardcore by my ballet teachers. To the point that I thought that I was a bad person for pronating my feet. (we were also made to feel bad about having to go take a pee in the middle of class, so I held my bladder a lot back in tose days… I think I wrote about that in my book Dance Stronger)
Here’s the paradox: Can a movement deemed “bad” happen at the same time as another movement that is “good”? And if yes, then does this make the good movement more bad? Or the bad movement more good?
Neither. They both just happen. No need to place any meaning or judgement.
To give you an idea of the stuff we recognize as “good” that happens when the foot pronates:
Glutes load (leading to a glute contraction that then extends the hip)
Plantar fascia and all muscles under the foot load and stretch and then help your foot supinate
Vastus medialis gets to do something useful (decelerate knee flexion)
TMJ decompression (as we are focusing on today!)
And more.
On the flip side, there are many other joint mechanics that couple with foot pronation are generally deemed “bad” for the body. A few of such terrible movements are:
Pelvis anterior tilt
Knee valgus
Spine extension
Hip internal rotation (although perhaps only in the dance world… we love to hate on hip internal rotation)
But remember, please, none of these movements are inherently bad or good. They simply happen.
What makes a movement better or worse for us is if it is happening too much, too fast, at the wrong time, or we get stuck in it as our only option.
Pronation is a like visiting Walmart. You want to get in, get what you need, and get out.
When we lable a movement (or anything…) as bad its often because we don’t understand it in its proper context, so our solution is to try to minimize, avoid, or control it.
Real freedom isn’t reached by controlling and manipulating our bodies, selectively avoiding entire movement spectrums. Just a little perceptual recalibration is required.
Let’s follow the flow (Motion Model)
In theory, using the Flow Motion Model, one can look at any bone or joint and, based on its position and velocity on the space-time continuum (if one can really measure both simultaneously…), one could extrapolate what the rest of the body should also be doing at that time moment in time. I think that’s pretty cool. Useful, too.
This is how we are able to make the connection we’re interested in today: Foot pronation couples with TMJ decompression.
If you’re up for it, join me now for a delightfully logical adventure through the body, joint by joint, from your foot to your face, linking foot mechanics to jaw mechanics.
I hope to highlight how movements like pronation and pelvis anterior tilt, which somtimes get a bad rep, are coupled movements. “Coupled” meaning that we want to see them happening at the same moment in time in gait.
Heel strike and away we go…
Let’s start at the beginning…
Which isn’t always so easy, even for a president.
… with the moment your heel hits the ground, and follow your foot as it rolls into it’s most nicest, flattest position.
For simplicity, we’ll call this moment in time pronation, and we’ll defnine it as the one chance your foot gets to pronate on the ground in gait. Its the moment in time at which many mechanics of shock absorption spring into action (get it??).
Let’s keep things super simple and define our pronating foot in terms of pressure, shape, open vs. closed joints, and long vs. short muscles.
As your foot fully pronates in a healthy way, and hoping it can maintain three points of contact- on the 1st and 5th metatarsals and your heel- you should notice the following:
Pressure on the foot travelling anterior and medial towards the 1st metatarsal joint.
All foot arches lowering and spreading, foot shape is becoming wider and longer.
All joints opening on the plantar/medial foot, and closing on the dorsal/lateral surface.
Muscles lenghtening on the plantar/medial surface, and shortening on the dorsal lateral.
A slide from day 2 of my Liberated Body workshop
And all the reverse mechanics happen as the foot supinates.
Pronation of the foot should happen with knee flexion. Let’s check if that joint interaction is naturally present for you.
What’s happening at your knees? If you stand on your two feet and bend your knees, without trying to do what you envision the perfect version of a knee bend should be, do feel your feet naturally pronate, as described above? How do your feet naturally respond? Has your training, like mine, been to avoid pronating your feet? And whait happens if you suspend that belief about pronation being wrong?
If you had no prior information about what SHOULD happen what do you feel IS happening?
If your foot pressures are going the opposite way- lateral and posterior towards your heels, what does it feel like to allow the pronation to occur?
Yes, your knees may go slightly inward. A little bit is ok. A lot is not. Embrace your right to valgus in this moment. The real money is when you don’t need to use a knee valgus to pronate your feet.
What’s your pelvis doing? As you bend your knees and pronate your feet, are you doing a pelvis anterior or posterior tilt? We’d like to see an anterior pelvis tilt. Why?
Feel this out: As you anterior tilt your pelvis, notice how this internally rotates your femurs, tibias, talus(es), and all that internal rotation should contribute to both feet pronating (talus IR is part of foot pronation).
If you do a posterior tilt with your pelvis, you drive supination mechanics via an external rotation of all those leg joints. Maybe posterior tilting is a good way to avoid pronation. But also, maybe you don’t need to avoid pronation?
Also note there are two ways to anterior tilt the pelvis, and only one of them is useful in gait (watch the video below…)
What’s your lumbar spine doing? As you anterior tilt your pelvis, what is the natural, uncsonsioud response at your lumbar spine? We know that as the sacrum nutates with the whole pelvis anteriorally tilting, the lumbar spine will follow into extension. But what does YOURS actually do? Also consider, does it feel like you use your lumbar extension to anteriorally tilt your pelvis? Or does your pelvis anterior tilt lead to a nice extension of your lumbar spine?
What’s your thoracic spine and ribcage doing? As your lumbars extend, does that extension continue to flow up into your thoracic spine, tilting your ribcage up and back (posterior tilt)? Should do! Unless you have a restriction blocking that spine wave up.
What’s your cervical spine and skull doing? Keep your eyes on the horizon, stand on your happily pronating feet, and notice, with spine extension, what motion do you feel happening in your neck? Does your chin lift up and extend your neck? Or do you feel your chin drop and your neck flexing?
Hopefully you feel your kkull anteriorally tilting and your neck flexing. Occipital atlantal joint decompressing.
And finally…
What’s your jaw doing? Remembering that your mandible is a dangler, let it dangle as you tilt your entire skull anteriorally, with your spine extending underneath. Which way does your mandible slide? Forward and down (protrusion/decompression from temporal bone) and dangling further from your face? Does it retract back in towards your face? Or does it do nothing?
Ideally, what you’d like to feel is the jaw sliding forward. Decompressing. If you try to keep it retracted it will seriously block your ability to flex your cervical spine. Just try it!
Do you have all these links in the chain? Or are there some blocked interactions?
If that was too wordy, I invite you to follow this adventure guided by me! Here’s a clip from the session last week in which we did this exploration.
How’d that go for you? Got all the links in the chain? Would love to hear what yo uobserved.
And if that wasn’t so smooth and flowy for you, what do you do about it? Perhaps you’d enjoy my workshop, Liberated Body. which I am now teaching online via the ubiquitous Zoom. Liberated Body is all about finding the missing links in your own body, and restoring them to have a richer experience of your body.
The next workshop is coming up in a few weeks on June 27th. Tell yo’ friends.
Until next time, my fellow body mechanics detectives 🙂