Raise your hand if your neck and jaw feel fantastic right now (honestly, mine feels a little like s#!te). I am going to assume your hand is down…
I’d like to share a 9 minute movement exploration to help you find a little more space in your neck, reduce tension and gripping in your jaw, and stand with your head in a better alignment over your body. Instead of like this:
If you’re feelin’ shrimpy, clear a spot on the floor and follow along with me:
I use this exercise with my clients who have limited neck range of motion, compressed (retracted) jaws, jammed occiputs, and even migraines.
Who should do it?
Most humans who stand upright on two feet within Earth’s field of gravity will enjoy this exercise. Particularly if:
You have a forward head posture.
The muscles at the back of your neck and upper traps feel hard and constricted and tight.
Your jaw muscles always feel clenched and sore.
You grind your teeth at night.
You get muscle tension headaches.
You feel like your shoulders are always up to your ears.
You’re like me and all of your life stress manifests itself in your neck and jaw.
You’re like me and you’re constantly smiling in an attempt to overcome crippling social anxiety.
When to do it?
Anytime!I personally like to do it as part of my morning movement practice and before and/or after I do any deliberate movement/exercise. You might like to use it to break up bouts of sitting so you don’t become a stagnant clump of spineneckjaw (how I feel right now). Or use it to relax anytime you notice tension building up.
I hope you enjoy this little movement exploration and found it useful for helping your neck and jaw (and life) feel more chill.
If anything about this movement feels uncomfortable or bad in your body, don’t force through it. Not everyone needs this exercise. If you have questions, please ask!
Want more help for your neck?
You may enjoy my Movement Deep Dive session: Check Your Neck.
Learn how your neck moves in relation to the rest of your body in gait.
Self- assess your neck
Explore movements that give your neck back it’s missing options for healthy ranges of motion.
And if you’d like more personalized guidance, shoot me an email or a DM on Instagram or Facebook, and we can talk about how to get your body feeling and moving better.
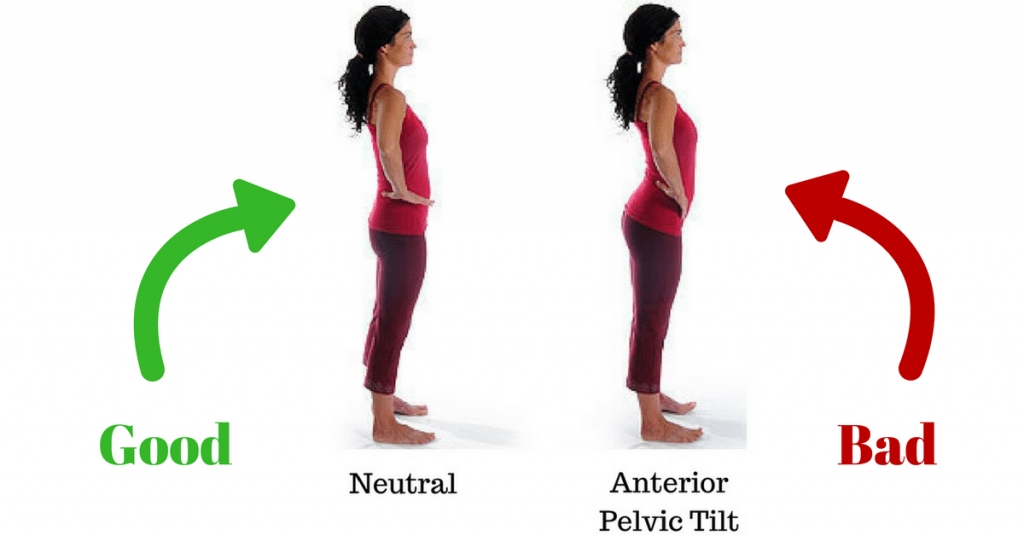
So, your trainer/physio just told you you have an anterior pelvic tilt that needs to be corrected because it’s bad. OMG. You’re doomed! Right? Or… Maybe not? Is an anterior pelvic tilt actually bad? And posterior tilt good?
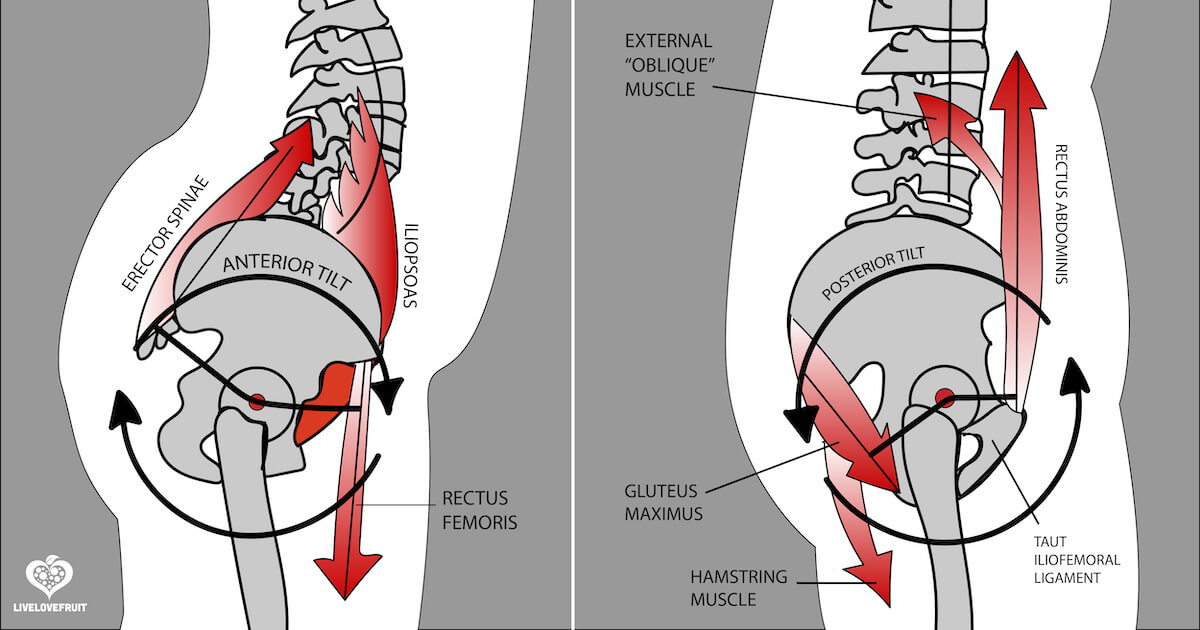
On the left: Anterior pelvic tilt (tailbone lifts up) On the right: Posterior pelvic tilt (tailbone tucks down)
Repeat this as your mantra: There’s no such thing as an inherently good or bad movement.
Have you ever been told that you have the dreaded “anterior pelvic tilt”? And it’s the cause of all your body’s problems? I have. And I believed it, too.
Most of us have been taught that some movements are universally “bad” and we need to fix them. Anterior pelvic tilt is nothing more than three words describing a movement a healthy body should be able to do, not a life sentence to pain, misery, and moral judgement.
Don’t listen to Dr. Google
I did a Google search for the neutral term “anterior pelvic tilt” and the first result tells me it’s something I should care about correcting! WHAT??! What if I didn’t even know what a pelvis is, and now the first thing I’ve learned is that mine might be wrong…
Just check out these results from the frist page of Google:
If you’re a pilates teacher no doubt this was drilled into you
Just a sampling of fix-yer-dang-pelvis-AT fear-mongernig from first page of Google
Contrary to what you may read from Dr. Google about fixing your pelvis AT, any movement we avoid (deliberately or unconsciously) will limit us. Labelling movements as “bad” and avoiding them, our bodies will, ironically, become less free, less efficient, less flowing (and less fun!).
Pelvis anterior tilt is but one example. Another one is foot pronation. So is shoulder blade (scapula) protraction.
I, Monika (trust me, I’m a movement proefessional), hereby give you permission to do all of those things with your body, not that you need permission. In fact, I ask people to reclaim these “bad” movements in my Liberated Body Workshop.
Does an pelvis anterior tilt need correcting?
Now you know: No. Your body needs to be able to do an anterior tilt well, and do it with every step you take.
And there’s more to an anterior tilt of the pelvis is more than jamming your tailbone up to the ceiling. If it hurts your lower back to do an anterior tilt, you’re probably doing it wrong. Don’t avoid it, learn how to do one well.
Why?
You need an anterior tilt to load your extensor chain (glutes and hamstrings).
You need an anterior tilt to absorb shock through your hips and spine with each foot step.
And, you even need your pelvis to do an anterior tilt well if you want your jaw to be able to decompress. (Do you wear a night guard for bruxism? Hmm, maybe you’d like to assess your pelvic tilting as part of a hoistic strategy?)
The idea we need to “correct” a pelvis anterior tilt because it is bad and causes back pain is just an idea that is based on an incomplete, compartmentalized understanding of the body in motion. We can do better.
The truth? We need to be able to do an anterior tilt WELL just as we need to be able to do it’s opposite- posterior tilt, well. BOTH matter for the health of your hips, spine, and well, your whole body (and your life).
Think of it this way: If you could only choose to turn left or turn right for the rest of your life, which direction would you choose? Is one better than the other? Or would you like to do both? If Zoolander taught us one thing, it’s the pain of living a life with only the option to go right.
“I’m not an ambituner… I can’t turn left”
Case Study
A few days ago I worked with a client with lower back pain. He is a former high level curler 🥌. His back pain feels worse when he does a pelvis anterior tilt.
Traditional thinking would have us believe that we should avoid anterior tilting his pelvis like the plague and get him to squeeze his butt and tuck it under, right??
Not so fast…
As you’ll see in the video below, he actually has HUGE amounts of pelvis tuck-ability (posterior tilt). Wayyy too much. And you’ll hopefully see how it is dragging his spine backwards behind his feet and into a ton of flexion.
I’d also like you to observe how his pelvis anterior tilt pushes his whole torso forward, like a tree tipping over, putting his head well in front of his feet. This is the movement that is flagging up his back pain because he is shearing forward from one segment in his lumbar spine, instead of evenly articulating across all joints to make a healthy extension.
Check out the analysis I did below: Pelvis tilts BC (Before Cogs)
https://youtu.be/5rlDViqaTtM
If you’ve been studying the newly released Anatomy in Motion online course from Gary Ward and co.: Closed chain upper body biomechanics in motion, then in the first chpater you will have learned that for healthy spine motion in upright gait we’d like to see your head stacked on top of your pelvis when it moves into AT and PT. Not swaying you forward and back like bamboo in the wind.
We call that stacked up pelvis on ribcage on skull organization on-axis. I also like to call it a shishkabob. Your spine is the stick. Mmm… Kebab…
In my clients’ case, his entire torso is being pushed forward by a pelvis anterior tilt, which shows us a few important things:
a) This person is not able to access an actual pelvis anterior tilt (and therefore there’s nothing to “fix”, it’s a movement to re-discover!)
b) This person probably has a imitation in intervertebral articulation into spine extension, which is needed to keep his head over his pelvis (actual movement between each individual joint in the spine, instead of being a tree trunk) This is important for spine health. And for giving the abdominal muscles something to do. Want abs? Add being able to anterior tilt to your list.
Now check out THIS second video, which I took after doing 10 minutes of corrective exercise to help him and his body re-learn what both pelvis anterior and posterior tilts with proper spine articulation feel like.
Pelvis tilts AC (AFTER Cogs)
https://youtu.be/EbxkPxqsMmo
Can you observe the cleaner pelvis and spine articulation, and less forwards/backwards swaying of his whole torso? He also reports no more back discomfort. Booyah!
What did we do?
Cogs: Our favourite exercise in AiM world. Which I’ve written about before.
Check out THIS video of me doing some floor cogs for an example of what I took my client through (or learn more in day 1 of Liberated Body with me :)).
And I can’t say enough about the Upper Body Biomechanics in Motion course, which has an amazing section on cogs if you’re an uber nerd and want the technical details.
Such a good course! I’m biased and I strongly recommend 😉
Now, what is important to understand is that in the AFTER video, my client is not consciously trying to do “good” pelvis tilts because he now knows what it should look like.
I’m not saying, “Hey Bob, based on what I told you about pelvis motion, can you make that happen with your mind-power?”
I’m asking, “Hey Bob, show me what happens if you ask your body to tilt your pelvis both ways without over-thinking how you’re doing it”.
Can you appreciate the difference?
This is a representation of his body having better unconscious access to a new way of moving that takes LESS control, less forcing, less micromanaging, and less energy. More likely to happen naturally in each step.
What are the take-aways?
If anyone tells you that a movement is bad, don’t believe them. BUT, sometimes movements can become unhealthy- asymmetrical, excessive, too small, too slow, too fast, unorganized with the whole, etc- then we need to re-train the bdoy how to perform it, coordinated with the rest of the body.
Whhile a pelvis anterior tilt was a trigger for my client’s back pain, the “fix” wasn’t to eliminate pelvis anterior tilt from his life. The problem was that he couldn’t do one at all, and was shearing from his spine too much, instead.
Too much posterior tilt can be just as much of an issue as too much anterior tilt. My client in this post is is case in point.
We need our bodies to be able to access both posterior AND anterior tilts of the pelvis. Remember Zoolander.
The better we become at observing movement, the better was can get at finding solutions that help us reclaim our options for moving better.
So… how well can your pelvis move? 🤔
Want to learn more?
Movement myths abound in the worlds of fitness and therapy.
Knowing what a human body should be able to do and having a safe, non-judgemental space to explore how your body moves so you can understand what healthy movement feels like for you is so important for getting out of pain and optimizing performance.
Want to learn more about optimizing how your body moves, based on gait and the teachings of Anatomy in Motion? This is the kind of things I help folks with in Movement Detective School .
If you’re ready to stop wasting time with generic exericses and stretches, and you’re serious about learning how to undo the patterns you have adopted over the years due to past activities, sports, repetitive postures, injuries, and accidents, I’d love to work together on that 💪
I’ve dedicated the past 10 years of my life to learning how to get my body out of pain by exposing it to the truth of how our bodies move in gait, and I have so much about that process to share. Shoot me an email if you have any questions 🙂
Fancy a little movement detectivery you can do for free, from the comfort of your own home?
Well, not completely free… You need the internet (and I don’t know about you, but my rates just went UP!). And you’ll have to stand up and use your brain and your muscles a bit, so it might not be as comfortable as sitting on your butt.
Regardless, if you have jaw issues, hip issues, or both issues, I think you’ll appreciate this little piece of biomechanical investigation. The video below is a simple way to test if your jaw’s resting position (which may be a lil’ off center), is messing with how your hips and pelvis are able to move.
Can you see how when I shift my jaw one way it makes things looks really discombobulated? What’s up with that huh?
The Jaw vs. Hips Test Explanation
In this video I’m testing if the resting position of my lower jaw (mandible) is impacting on my ability to hike my pelvis on either side (and thus adduct/abduct my hips- which needs to happen with every step we take for efficient gait).
Ideally, our pelvis hikes and drops with each foot step we take. We also want our bodies to move as evenly as possible on the right and left sides: Pelvis hike on the right should be pretty dang close to the hike on the left.
In this assessment, we’re looking clean and clear (and under control…) frontal plane motion, meaning purely up and down motion. Not a pelvis rotation. Not a pelvis thrust. Pelvis bones ought to move like elevators, not a washing machine.
In this assessment, pelvis hiking is accomplished by gently bending one knee to allow the opposite side of the pelvis to hike up on it’s own. I’m not trying to use my side-abs to pull my pelvis up with a muscular contraction. This is an assessment of how your pelvis reacts to a knee bend, NOT trying to see how high you can jam your iliac crest into your ear like it’s a contest.
Start by evaluating how each side hikes with your jaw doing it’s natural thang. Note any differences. This is your baseline.
Next, slide your jaw to the RIGHT (like a type-writer). Repeat your pelvis hikes. Notice if that changes anything. Better, same, or worse?
Lastly, slide your jaw to the LEFT. Repeat your pelvis hikes. Notice if that changes anything. More even right and left? Less even? Any discomfort?
Did one of those three jaw positions make your pelvis hikes more even? More comfortable? Worse? Or no difference?
The Results
If you are perceptive, you can probably see which jaw position helps my pelvis and hips achieve more balanced, clean motion.
(FYI my right and left sides are reveresd. My tattoo leg is my right leg…One of my online students actually remarked that it was great to have my right leg so clearly denoted because it helps her keep track of the rights and lefts in class! Yes… I got that tat for exactly that reason… ;))
Here’s the video again, to save you some scrolling:
Round 1: Jaw in it’s default resting position. My pelvis hikes look pretty even right and left, eh?
Round 2: Jaw shifted LEFT. When I hike left side up, I shift off of that leg. And when I hike right, I rotate towards the right instead of hiking. This is NOT clean motion, meaning I have poor access to both pelvis hikes.
Round 3: Jaw shifted RIGHT. This looks very similar to round 1, but in my body it feels smoother and happier.
So, if I had to pick one jaw position that promotes optimal hip motion, jaw shifted right is the winner.
Interpretating the Results
Okay, so what’s the point of this, and what, if any, useful information can we glean from it in the name of better, pain-free movement?
Jaw position is kind of a big deal.
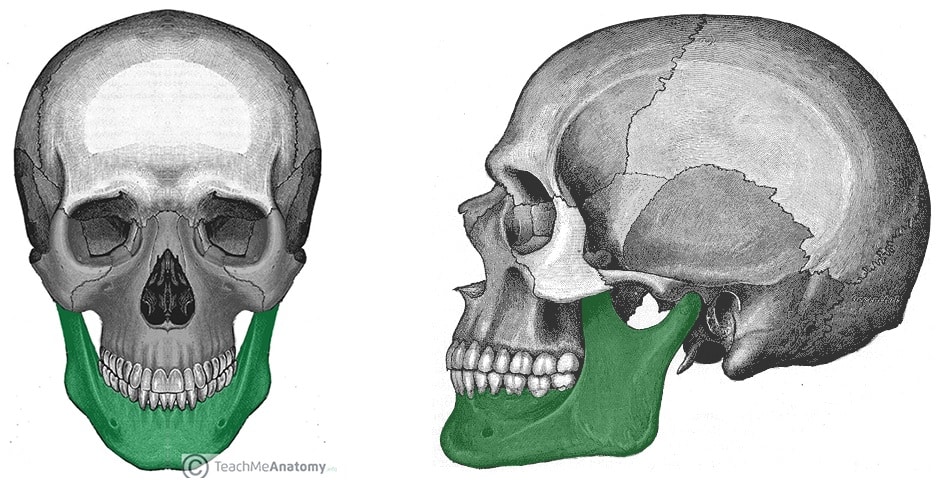
Interestingly, our mandible’s position in our skull dictates a lot about how we’re able to move our hips and pelvis in gait (among other things… THAT’S a rabbit hole of a lifetime that will make you very disappointed in humanity and yet empowered to pay attention to your oral-facial health and tell everyone to shut their dang mouth while they breathe. But don’t get too high on that soapbox…).
We can consider the jaw to be a “leveller” of the body- A mid-line structure with a significant impact on whole body mechanics. What if your body took part of it’s cue for where its center is, based on where your jaw is? What if this had an impact on which phases of gait you can and can’t access (it does)?
So when you notice your jaw is “tight” or clicky or you clench it, know that this is not just a jaw problem- It’s a whole body problem.
What I haven’t mentioned yet is that my jaw’s default resting position is already shifted to the left.
So in round 1 of the test, my jaw is actually sitting slightly left of center. I think it’s been that way since I was at least 3 years old. Why do I think that? Because I have a photo of me on my third birthday in which my jaw looks like it’s pushed farther back on the left side.
Like this:
Its subtle, but can you see the left side of my jaw shoved back farther than on the right? Happy bday to me!
In round 2 of the test, when I slide my jaw to the left, my pelvis and hips have no clue how to move in the frontal plane! What’s going on here?
As mentioned earlier, hiking the pelvis needs to happen with each footstep. It’s part of our bodies’ shock-absorption mechanics that happens when our foot pronates on the ground, loading the lateral glutes medius and minimus (this is suspension phase of gait for the AiM folks, loading phase for the rest of y’all).
So too does the jaw have it’s own coordinated movement with the whole body in gait for optimal efficiency.
In gait, when the pelvis hikes on one side, the jaw actually needs to slide over and gap (teeth come apart) on that side as part of a whole body pattern for efficient movement.
In another moment in gait, when the right heel hits the ground (heel strike), the jaw actually shifts to the left. Interestingly, right heel strike is a phase in which I experience right hip and SIJ pain sometimes. In fact, right hip pain was the first chronic pain symptom I ever remember having.
So this gets me thinking… How long has my jaw been messing with my hips? Has my resting-left jaw tendency predisposes me to having the hip problems that I did/still do? Have my hips really been on a path of destruction since I was three years old (or even earlier?). I don’t think this is random, or coincidence…
What do you do with this new data?
Let’s say you’re like me, and if you shift your jaw left your pelvis doesn’t know the meaning of “hike”.
Let’s look at the data:
Where’s my jaw at rest? Shifted left.
When I shift it MORE left (deeper into default) I can’t hike either side of my pelvis, when I shift it right, things improve.
Thus my jaw being positioned left is highly likely to be giving my hips and pelvis some grief
Solution? Getting my jaw to not be stuck to the left all the time and have a more centered default position would likely have a beneficial whole body effect.
The journey from here- what you decide to do, will vary based on the tools you have in your toolkit to reorganize your jaw. Manual therapy, movement re-training, goofy looking face stretches, all can be useful.
For the past 3 years I’ve been on a journey of levelling my jaw. It’s been a fascinating, enriching, and frustrating project.
Here are a few interesting things I’ve noted along the way that have helped me un-leftify my jaw, and significantly improve how my hips feel:
I prefer to unconsciously chew on the left side. It’s my happy place. I try not to always chew in my happy place.
When I am in social-anxiety-producing situations, I unconsiously clench my jaw and shift it to the left. It’s where my jaw goes when I’m trying to cope with stress. Now I’m at the point that I’m conscious of it happening. Sometimes I can even NOT DO IT.
Oral-facial integration techniques (a la MNRI) and craniosacral therapy have been super helpful for me. I can do these manual therapy techniques on myself because our faces are easily within hands-reach. Learning these two modalities have been game-changing.
Understanding how jaw motion couples with the rest of our bodies in gait, as per the Flow Motion Model taught by Gary Ward in his Anatomy in Motion courses has been crucial for me to use whole body movements to re-integrate my jaw with my body in a meaningful context, i.e. walking. Do you know what your jaw should be doing in three dimensions with a pelvis hike? Well mine isn’t doing the right thing! And reorganizing that has been key.
I used to get weird popping and ringing sensations in my left ear, especially under stress… Now they are almost gone, but come back when my jaw is more to the left (which happens when I’m under stress).
Making funny faces is an awesome and important part of changing the way you move 😜 I mean, this is serious business, but that doesn’ t mean we can’t have some serious fun with it.
My invitation to you
Are you feeling like a Movement Detective? This is the kind of stuff I like to share with my students in my secret Movement Detective School. Oops, not so secret anymore…
Give this test a try and see if your jaw could be impacting the motion of your pelvis and hips.
It is quite likely you have one position in which your jaw discombobulates your hips.
Is that the same side you have a clicky, poppy jaw? Is that the same side you chew on primarily? Is that the same side you got smoked in the face by some aggressive jerk in a hockey match? Is that the same side you had a traumatic experience getting your wisdom teeth removed?
Let me know what you find. What if you could free your jaw, free your hips, and free your life? (you can!)
PS I share little videos like this from time to time on my Instagram page. I think social media sucks 90% of the time, but I like to use it to share the nerdy movement things that I do. Feel free to follow me @monvolkmar
December 18th was this month’s edition of the Movement Nerd Hangout: A free monthly session to welcome you into my wee community of self-professed movement detectives (aka movement nerds).
This month’s topic was Core Training From the Inside Out (part 1). I figured everyone’s thinking about their mid-section around this hedonic time of year, so yes I jumped on that marketing train. Sue me.
Over 100 lovely people signed up to explore some rather unconventional concepts and ways of experiencing their “core”, such as:
What is core mobility vs. core stability? (and why this may be the missing link to building a strong core)
How could ankle sprain rehab be considered “indirect” core training?
What’s your center of mass (CoM) awareness got to do with core training? And how is it more important than a “neutral” spine?
What the heck is “neutral spine” anyway? Should you work on it?
How does Gary Ward’s rule of motion: Muscles lengthen before they contract, come to life in a diaphragmatic breath, as it relates to training dem abz?
How does access to 3D spinal mobility actually improve core stability?
And more…
In case you missed the live session, here’s the complete recording:
Carve yourself out an hour to hang out with me and dive into my first two pillars of core training. Let me know how it goes for you!
And now, here’s the session breakdown, if you just want to read some words, or don’t have time to participate right now.
Core intentions
Here is what I set out to cover in the session:
Understand what is “the core”? And identify the key anatomy.
Understand and explore my first 2 (of four) pillars (that I made up) of core training: 1) Diaphragmatic breathing at rest, and 2) Accessing 3D spinal motion.
Apply Gary Ward’s two rules of motion: 1 ) Joints act, muscles react, and 2) Muscles lengthen before they contract, to core training, in contrast to “core stability”
Whoah what? A core training session that’s NOT about creating stability and engaging your abs?? But isn’t the core supposed to be stable??
We’ll get right into that, but let’s first look at some of the key anatomy.
Core anatomy
What is the core, anyway?
In the session, I asked participants: “Point to your core”.
Do it now… What are you actually pointing to?
Are you pointing to muscles? Are you pointing to your ribcage? Are you pointing to your intra-abdominal pressure? Are you poining to your center of mass? Are you pointing to your breath?
The core is all of that, and more than all that. It is how all of that interacts.
The core is more than a set of muscles.
More than a label of weak or strong. More than something to squeeze, tighten, and brace. It’s more than stabilizing your spine. More than something to tone and make look good. And not something we need to dedicate a whole gym day to.
But I digress… Let’s take a look at the key muscles, bones, and joints of the core.
Key muscles & structures
Bones and joints:
Pelvis
Ribcage
Spine
Consider the muscles that attach from ribcage to pelvis, spanning the length of the spine
Muscles (that connect directly to those bones and joints)
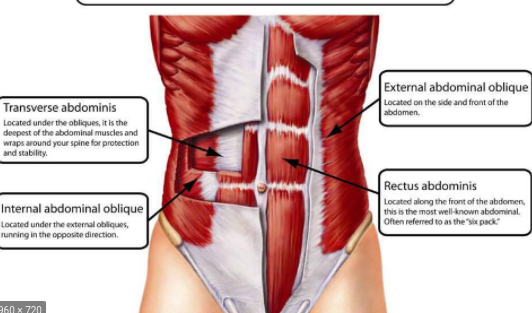
Rectus abdominis
Internal obliques
External obliques
Transversus abdominis
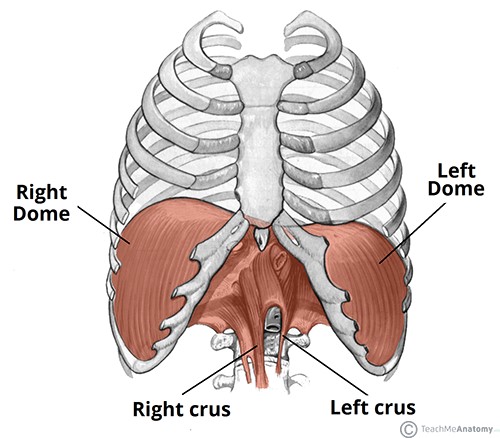
Diaphragm
Multifidus and other inter-vertebral muscles
*Note, however, we won’t be talking specifically about muscles today, because it’s actually not that useful experientially, and makes things way more complicated than necessary.
Voila les muscles.
And the diaphragm, attaching from ribcage to spine. Contracts with inhalation and relaxes wtih exhalation.
These structures and muscles all have a specific role in gait.
What does the core do while you’re walking?
WHEN does it contract? HOW does it contract? Should you even think about contracting it while you walk? (No…)
The abdominal muscles are no different than any other muscle in motion: They go through phases of loading/contraction, lengthening/shortening, as the joints they attach to go through phases of opening/closing, compression/decompression.
This all happens multiple times per foot step, in all three planes of motion.
While I don’t say it explicitly, day one of my Liberated Body workshop (spine mechanics day) could be considered a “core training” session, because it’s all about experiencing spine, pelvis, and ribcage movements as they occur harmoniously in gait.
Within the fraction of a second it takes for each foot step, all the structures of the core lengthen then contract, compress then decompress, in all three planes.
Gait might be the best core “workout” you can get 😉
So… Can you appreciate that core training is about more than just stability, six packs, and neutral spine?
“Direct” and “indirect” core training
This is something I made up, so take it with a grain of salt. But I’d love to hear if it resonates with you as a concept.
I’d like to poropose two types of “core training” (neither of which involves stability, or romanticizing neutral spine):
Direct (or local)
– Working directly with the spine and trunk musculature, the position/movement of spine, pelvis, and ribcage, and the ability to breathe within all options for those positions/movements.
– The potential for the structures named above to alternate between demands for movement or creating stiffness, in a way that is effective for the current task.
Examples of direct core training: Working directly on spine mobility. Doing core stability exercises, like deadbugs. In real life, being able to brace the abdominal muscles, create a rigid spine, and maintain intra-abdominal pressure in order to push your car uphill.
Indirect (or global)
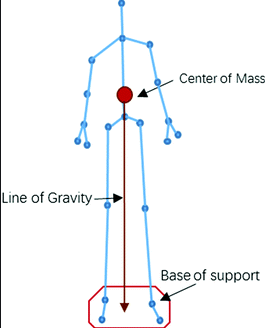
– Freedom for one’s center of mass (CoM) to move freely within the base of support of your feet, to all it’s edges. The ability to find your best “center”, having explored those edges, instead of forcing an idea of neutral spine on a structure lacking awareness of center.
– CoM mobility (or “core mobility”, a term Gary Ward coined in What the Foot) gives rise to the core musculature (and all musculature) reflexively responding, unconsciously, as the body moves.
– Indirect training is specific to the individual based on their unique history- Injuries, sports, habitual patterning and postures. Indirect work is to give the whole body back “what’s missing”, knowing it will impact on how the core functions.
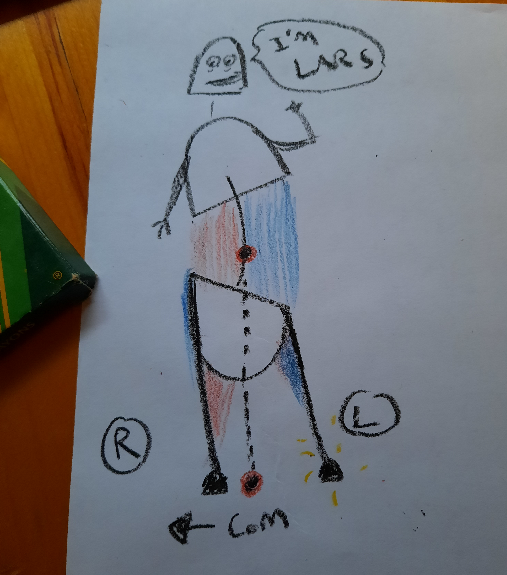
Example of indirect core training: I’ll use an example of one of my clients. I’ll call him Lars.
Lars had a left ankle sprain, and now he can’t bend that knee very deeply, and he can’t get his body (CoM) over to his left foot.
He looks a little like this:
Another Monika Volkmar original
Lars has left side SI joint and lower back pain, and does a ton of core stability training, because shouldn’t stronger abs help with your SIJ and back?
Not if the problem is that you can’t put weight on your left foot, which is the case for Lars. He can’t shift his center of mass left without weird compensations in his spine and pelvis.
All the blue shading is where muscles are getting pulled long, which are the areas he feels “tight”.
He is very good at training his abs in his off-center place- He’s got a very “strong” core. But it is not helping him to liberate his mass to move freely from one foot to the other, only serving to further lock him into an off-center structure.
As we’ve been working on his left ankle and knee, his pelvis and spine are balancing out, helping him to use his abs better, from a more centered place, because he doesn’t need to lean away from his left leg so much.
So yes, core training is absolutely about the spine, and muscles (direct).
And its also about the whole body’s ability to move freely, not avoid motions that feel unsafe due to past injuries, accidents, or trained movement patterns.
Lars’ ankle and knee movement training was indirectly giving him better access to his core, as he began to inhabit a more centered structure.
Ok now finally onto pillar #1…
Core Training Pillar #1: Diaphragmatic breathing at rest
This is my first “pillar” of core because a good quality diaphragmatic breath:
Descends the diaphragm, smooshing down on your guts, which is necessary to generate intra-abdominal pressure so you can be strong AF when the demand arises (pillar 3)
Mobilizes the spine, pelvis and ribcage (pillar 2)
Lengthens all the abdominal muscles- A good indicator of their ability to then reflexively contract (Gary Ward’s rule: muscles lengthen before they contract)
Has implications for many, many physiological, neural, and esoteric things that are fascinating but beyond the scope of “core”
I really enjoy this animation of the biomechanics of the diaphragm, and the effect of diaphragmatic breathing on the whole body:
To make things very, very simple, in the session I demonstrated a 5 quadrant quick check for your quality of diaphragmtic breathing:
Sternum and belly anterior (aka apical) expansion
Lower pelvis anterior expansion
Upper chest (aka pump handle ) expansion
Lateral ribcage (aka bucket handle) expansion
Posterior ribcage expansion
Are you able to access all 5? Are you all belly and no pump handle? Or are you like me and your left ribcage bucket handle never moves?
All 5 quadrants expanding simultaneously, effortlessly, and unconsiously is a good indicator of a quality diaphragmatic breath.
Core Training Pillar #2: Access to 3D spinal motion
First remember: Core training isn’t just about stabilizing and neutralizing the spine.
Second remember: Your spine moves when you walk (well it should, but maybe yours doesn’t… yet!.)
Third remember: Muscles lengthen before they contract.
Fourth remember: Joints act, muscles react.
So as a prerequisite to having abs that can contract and create stability, we need access to the specific 3D spinal motions that occur with each foot step you take:
Sagittal plane: Flexion and extension.
Frontal plane: Lateral flexions left and right.
Transverse plane: Rotations left and right.
In the session we covered a few exercises to experience the sagittal plane motions: Flexion and extension of the spine. And as a bonus we layered on the 5 quadrant breathing.
Greater access to the whole spine’s movement potential acctually gives you greater ability to stabilize it, too.
To help participants experience this, I had them test out a plank (holding for ~5 breaths), and gauge how “stable” they felt.
Then after exploring some spine motions, I had them re-test their plank. Here are some of their reactions:
“2nd time felt much stronger, more stable and able to access my breath more fully”
“Foot pressure balanced out – started really far on the left foot – more balanced. Also much more stable plank :)”
Pretty cool, eh?
Conclusions?
“Core” can mean a lot of things. What does core mean to you?
Many folks start core strengthening and stability training from the “outside in”, before considering the “inside” part: Breathing, spine motion, and center of mass mobility.
Ankle sprain rehab can be considered “indirect” core training, because it can give you greater access to move evenly between your two feet, aka “core mobility”, or “finding center”.
Neutral spine only lasts a fraction of a second when we walk- A fleeting moment in time.
Diaphragmatic breathing is not belly breathing- There are four other quadrants that need to expand with the belly with every inhalation. How’s yours doing?
Giving the abominal muscles the experience of how they actually lengthen and contract as we walk, by accessing three dimensional spine motion, should be the first poriority for core training, before training for stability.
Want to tune in live for part 2?
Save the date: Wed Jan 27th 2021 @ 10:30am EST (Torono)
In Core Training From the Inside Out )Part 2) we’ll review the first two pillars, and dive into 3 and 4:
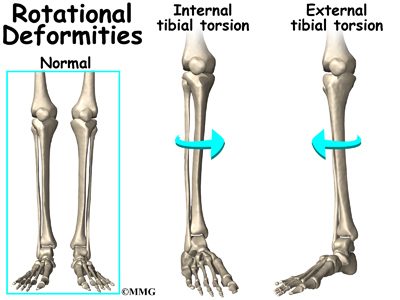
Last week I saw three different people with externally rotated knees. In particular: Three externally rotated right knees that don’t internally rotate, causing the individual some grief (not just at the knee, but definitely at the knee).
These “deformities” actually happen in gait… I guess we’re all deformed.
I remember Gary Ward saying something to the effect of, if you keep seeing the same thing over and over again in your practice within a short period of time, check to see if it’s not your OWN issues that you’re projecting onto your clients. Have been guilty of that in the past.
Just to make sure I’m not full of shite, I stand up, check out my right knee, and, lo and behold, it appears my right knee doesn’t fully internally rotate. Actually, both don’t. Well damn. However, my right knee internally rotates a lot more easily than my left, so, maybe my awareness, despite my imperfections, is helping to keep my perception honest. In any case, the important lesson: Whenever you see a bunch of the same thing, check to make sure it’s not just YOU.
I would like elaborate on a few observations I noted in working with these three individuals, aka, how not being able to internally rotate a knee can potentially wreak havoc on the body.
Some stuff they had in common, in particular:
Missing an effective propulsion phase of gait
Feet turning out in gait, aka, the “duck walk”
Rock solid, toned up, tibialis anterior
Low femoral external rotation
Limited right trunk rotation
Are you ready to get excruciatingly technical? Hell yeah!
LACKING PROPULSION
Propulsion- The phase in the gait cycle just before the foot picks up off the ground prior to swing in which the pelvis is travelling (propelling, if you will) forwards, the extending hip fully decompressing, and the foot is in a maximally supinated , rigid lever position. To create this rigid lever, the knee also needs to be locked in extension in order to anchor the foot to the ground so that the pelvis can travel forwards, allowing the hip to extend and load the hip flexors for the next moment: Swing.
Getting to propulsion effectively is important.
However, in all three of my funky-kneed individuals, propulsion was just not happening.
In propulsion, the knee will be in its end range of extension. For this to happen, the femur twists externally on top of the tibia, locking the condyles together into it’s “screwed home”, comfy position (home= comfy). This creates a position in which the tibial tuberosity is rotated medially of the femur, giving us an internally rotated knee.
Knee extension = knee internal rotation in an ideal situation in gait.
If the knee can’t get “home” to internal rotation and extension, as was the case for these three individuals, then the rigid lever to propel off of will be compromised, and resultant shite: The hip won’t extend, swing may be compromised, and all the muscles that load up in propulsion (psoas, iliacus, distal tibialis anterior, peroneals, distal hamstrings, distal FHL, adductors, to name some biggies), will not get their chance to lengthen.
Internally rotatable knees= Happy hips that can extend.
FEET TURNING OUT IN GAIT
That funny “duck” walk thing. I used to do that. And then I stopped ballet…
A little experiment you can try. Standing bilaterally, turn your feet out. Can you feel which way your talus is now pointing? If you are a normal human being, you should feel that feet out= sub-talar joint axis (STJ) pushes in. The opposite is true if you stand with your feet pointing inwards- STJ will point out.
Feet pointing out in gait is often a hint towards a foot that can’t pronate, and an attempt to give the STJ an opportunity to point inwards.
In pronation, the STJ axis will orient internally of the 2nd toe (usually wayyy more internally than that). But what if the foot can’t pronate? Or, what if pronation has become dangerous for some reason, and the body has needed to find a way to work around it?
Turning out the feet is one work-around: Feet out, STJ pushes in, medial arch gets to open, brain thinks it is “pronating”, but without actually pronating.
In gait, pronation and knee external rotation happen at the same time. This means that, in the case of the already externally rotated knee that doesn’t internally rotate, pronating the foot may feel dangerous because with the knee already externally rotated, there’s nowhere further to go if the foot pronates.
If the foot does pronate, the knee will reach end range external rotation (XR) too quickly and that may not feel so good. As a strategy, the body needs to find an alternative way to get a bit of “pronation” through the foot, and tan easy way to do this is to turn the foot out so that the talus can feel like it’s pointing in, and the medial arch can open. Not ideal. Definitely a work-around, but better than not being able to walk in the short term.
If the knee was able to internally rotate, this would free some space for it to move into external rotation as the foot pronates, rather than immediately crash into end-range. The change in timing allows pronation and external rotation of the knee to couple together safely.
In the case of these individuals, reintroducing knee IR was a foreign, but nurturing experience.
Tib ant is a cool muscle that I don’t completely understand. Its triplanar functions hurt my brain (and I still have to see some clients today who need it).
That said, I did spend about 20 minutes on my couch groaning in agony trying to make sense of tib ant, my room mate giving me strange looks (rightfully so).
Tib ant is a strange and fascinating muscle.
I believe it…
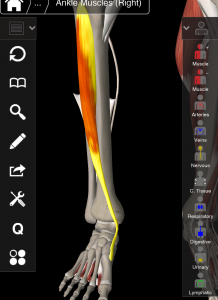
It lengthens and shortens at both ends simultaneously, despite being a multi-joint muscle (which generally do NOT do this unless you want it to feel really bad).
It shortens in two planes while lengthening in another, and visa versa (sagittal and transverse couple, while frontal opposes).
I enlisted a little help from some smart AiM friends to understand the closed chain mechanics of tib ant when the knee is interally vs externally rotated. Here is the verdict:
SAGITTAL: Long (except in strike phase of gait in which the ankle is actually dorsiflexed with an extended knee, and so the tib ant will be short here) FRONTAL: Short TRANSVERSE: Long
SAGITTAL: Short (note, this is passive shortening, as gravity does the job of dorsiflexing the ankle and pronating the foot.) FRONTAL: Long TRANSVERSE: Short
So, in the case of our friends with externally rotated knees and rock solid tib ant, what does this mean? Few theories for the increase in muscles density and hypertrophy:
Length tension: Being used excessively to decelerate a joint motion. For example:
Tib ant decelerates the arch lowering in frontal plane to manage over-pronation (aka shin splints). Slowing down pronation will serve an already externally rotated knee by preventing it from rotating further, and tib ant may be working overtime for this.
Ankle may be plantar flexing too quickly out of late swing in an attempt to decelerating sagittal plane ankle motion into dorsiflexion, and block over-pronation and thus, more knee external rotation.
Short, overworking tib ant: Concentric muscle tone. Some examples:
Not being able to lengthen and load tib ant in sagittal and transverse plane in the previous phase of gait, propulsion, the tib ant will have to contract excessively on swing to dorsiflex the ankle to clear the ground (or turn the foot out).
An externally rotated knee may be attached to a foot stuck in pronation and ankle stuck dorsiflexed, which will shorten tib ant in sagittal and transverse plane.
If a high varus angle of the foot is present as an attempt to slow pronation and knee external rotation (as this increases the distance the 1st met must travel before it hits the ground), this will contract tib ant in frontal plane.
I’m sure this is not a complete list. I am, of yet, not sure which one of these is the most true for each of my three individuals, but what matters more than the story I choose is the “what will I do next”?
LOW FEMORAL-ACETABULAR EXTERNAL ROTATION
In order for this to make sense, we must distinguish between femoral rotation (FA: femur moving in acetabulum), acetabular-femoral rotation (AF: acetaculum moving on femur), and hip rotation (the orientation of the space between the two bones).
Until I understood this distinction, and a lot of it has to due with timing, hip mechanics fucked with my mind. I blame PRI. Just kidding… I blame my limited thinking, conditioned by previous PRI training.
LEFT: Right AF IR, left AF XR. RIGHT: Right AF XR, right AF IR. I had to temporarily forget about this to learn AiM.
Moving on!
Curiously, in all three individuals, the right hip- the same side as the externally rotated knee, was more limited into external rotation than their left. Why could this be? (and yes I am aware that this is a left AIC pattern…)
When the knee is externally rotated, the hip can be either internally rotated (IR) or externally rotated (XR), depending on which phase of gait we’re talking about.
There are two phases of gait in which the knee does XR: Suspension and early swing. Both are pronating, and knee bending phases. The distinction: In suspension (closed chain), the hip is in XR, while in early swing (open chain), the hip is moving into IR from maximum XR.
In either case, if you were to freeze time at the moment the knee is in XR, the hip would appear to be in XR as well. In one case because it is really truly in XR (suspension), in the other, because it is still in a state of XR but moving into IR (early swing).
PLOT TWIST: In suspension, though the hip and knee are in XR, the femur in the acetabulum itself in internally rotating.
How can an internally rotated femur be labelled as externally rotating hip?
Here’s how:
Suspension= FA IR + AF XR + (*some timing stuff*) = Hip XR.
Remember the femur and the hip are not the same thing. The femur is the bone, the hip joint is the space between the femoral head and the acetabulum.
*Aforementioned important timing stuff*: In suspension, the pelvis is rotating away from the suspending leg (AF XR) as, just prior to hitting the ground, the leg was in swing. The leg swinging rotates the pelvis away from the swing leg (creating AF XR), as the femur also rotates externally (FA XR). Then, as the first met hits the ground and foot starts pronation, the femur begins to rotate internally, initiated by the talus as the foot begins to pronate. However, the pelvis is still rotating away (into AF XR) faster and farther than the femur is rotating internally, which creates a global position of hip external rotation.
Clear as mud, right?
Early swing, by contrast, is simple:
Early swing= FA IR + AF IR = Hip IR
So, when the knee is in XR, the femur IS internally rotating regardless of what the hip is doing. When the knee is in XR, the femur is internally rotated farther that the tibia.
Knowing this, it makes sense to feel a limitation in femur XR on the side that has an externally rotated knee.
This also makes sense as a contributing factor to why propulsion wasn’t happening: In propulsion we need hip AND femur XR along with knee IR.
LIMITED RIGHT TRUNK ROTATION
Having an externally rotated right knee and limited right trunk rotation are not an absolute coupling, but it was curious to see it in all three individuals this week. It was pretty interesting example of the clever body making adaptations above to accommodate something below (or is it something below adjusting for a structure above…?)
In two of the three, the same situation was going on:
In gait, both had an observable left trunk rotation. Ribs were going left-center-left-center, and never making it to the right.
BUT, in a bilateral stance, the opposite showed up: Both had an inability to rotate to the LEFT. What the f***. I was not expecting that.
Why would someone rotate left so much while they walk, but not at all when isolating ribcage movement in bilateral stance?
My operating theory is, what if they were already rotated left, and in which case, there is nowhere else to go. You can try this in your own body. Stand with your shoulders rotated to the left. Now, try to rotate them more to the left. Doesn’t get you very far, does it?
So why would the body choose to put its thorax to the left, and how does this relate to a right externally rotated knee?
Remember, knee XR happens twice: Suspension, and early swing. In both those phases of gait, the spine and ribcage will be rotating, wait for it….
TO THE RIGHT (as per the Flow Motion Model™)
What if the body is avoiding right spine rotation because the knee is already in end range XR? More right trunk rotation would potentially require the knee to XR further, and that would probably not feel good on an already externally rotated knee.
We can look at it from another perspective. Maybe the left trunk rotation is what is trying to create right knee IR. In all (but one) phases of gait in which the right knee is in IR (transition, shift, and propulsion), the spine will rotate LEFT. (the exception is right heel strike, in which the trunk will be rotating to the right, even though the knee is in IR).
So, right trunk rotation couples more with right knee XR, and left trunk rotation couples more with right knee IR.
So which is it? Using left trunk rotation to attempt to IR the knee? Or avoiding right trunk rotation to protect the right knee from excess XR? The answer will be “both” until we know for sure.
In any case, working on reintroducing right trunk rotation and right knee IR will be a nourishing experience. Hopefully… (so far so good).
CONCLUSIONS?
Yeah, I guess I have a few.
I’d better take care of my own right knee just in case I’m projecting my own problems onto people. Will put that on the to do list for today.
Is this right knee external rotation a PRI pattern? Part of the lef AIC pattern?
These three individual cases also had other different things going on. This is not the full picture and not meant to be taken as an absolute. I just like to write out my observations on the shit I see to make sense of it.
Part of the solution for all three of these individuals was to work on “transition” (AiM movement) to experience knee IR. All reported that it felt “weird”, “good”, and “I never do that”. No shit you don’t!
Knees are pretty cool. For a joint with only two planes of movement, amazing how overlooked its mechanics are. It only took me 4 times through AiM to start to get a grasp on the knee. Maybe after my 6th I’ll understand shoulders.
This blog post is entirely a thought experiment. None of this may be true. Take it all with a grain of salt.